
Cracked Tooth: When Can It Be Saved and When Does It Need to Be Extracted?
- Modern Dental Centre
- 12 hours ago
- 8 min read

A cracked tooth does not always mean the tooth is lost. But it does mean the clock has started because cracks do not heal, and most will progress without treatment. Whether dental extraction treatment becomes necessary depends entirely on where the crack is, how far it has travelled, and what structures it has already reached. Understanding those factors turns a confusing diagnosis into a clear decision.

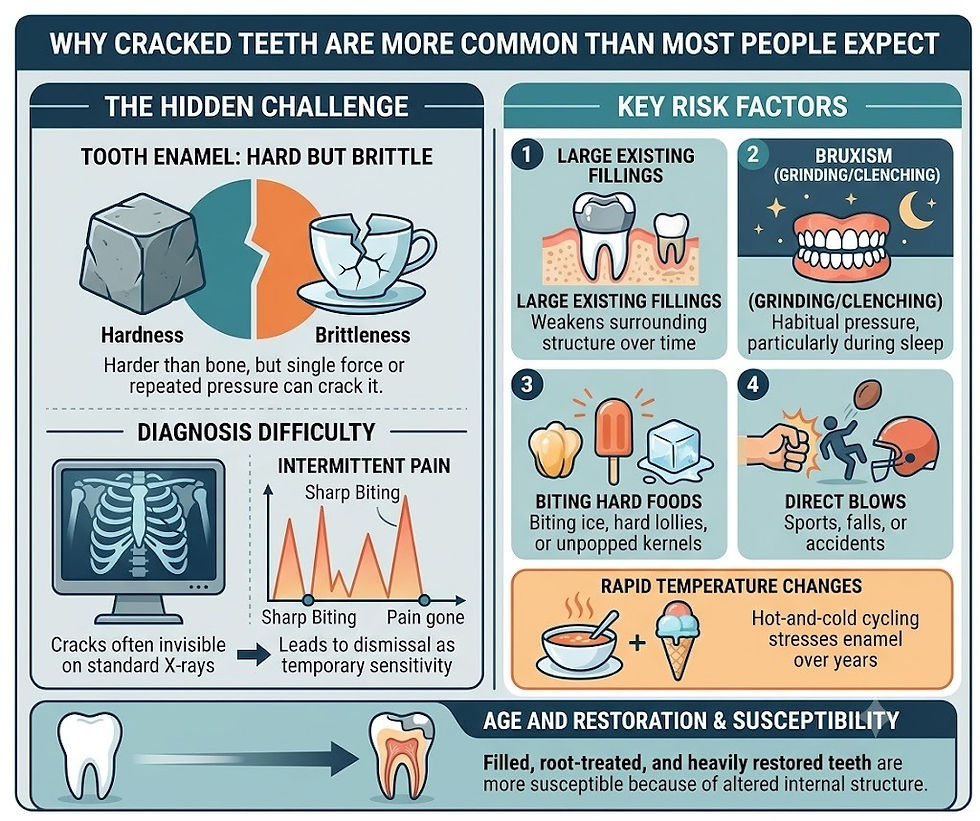
Why Cracked Teeth Are More Common Than Most People Expect
Tooth enamel is the hardest substance the human body produces harder than bone. Despite that, it is brittle. A single force applied at the wrong angle, repeated pressure from clenching, or years of temperature cycling from hot and cold food and drink can all initiate a crack that the naked eye may not detect for months.
The Australian Dental Association identifies cracked tooth syndrome as one of the most frequently misdiagnosed sources of dental pain, partly because cracks are often invisible on standard X-rays and partly because the pain they produce is intermittent sharp on biting, then gone, which leads many patients to dismiss it as temporary sensitivity rather than structural damage.
Several factors increase the likelihood of a cracked tooth:
Large existing fillings that weaken the surrounding tooth structure over time
Bruxism — habitual grinding or clenching, particularly during sleep
Biting down on hard foods such as ice, hard lollies, or unpopped popcorn kernels
A direct blow to the mouth from sport, a fall, or an accident
Rapid temperature changes — drinking something very cold immediately after something very hot stresses enamel repeatedly over years
Age is also a factor. Teeth that have been filled, root-treated, or heavily restored are more susceptible to cracking than intact teeth, simply because the internal structure has been altered.
The Five Types of Tooth Cracks and Why the Type Determines Everything
Dentists classify tooth cracks into five distinct categories. The category determines treatment, not the severity of pain which is why a tooth that hurts intensely is sometimes more salvageable than one that causes only mild discomfort.
1. Craze lines
Superficial cracks confined to the outer enamel layer only. They cause no pain, require no treatment, and are present in virtually every adult tooth to some degree. These are never a reason for extraction.
2. Fractured cusp
A crack that causes a piece of the biting surface the cusp to break away or become loose. The pulp (inner nerve tissue) is usually not affected. Treatment is typically a crown or onlay to restore the biting surface and seal the crack. Prognosis is generally good.
3. Cracked tooth
A crack that begins at the biting surface and travels vertically toward the root. This is the category that produces the classic cracked tooth syndrome symptom: sharp pain when biting that disappears almost immediately. The critical clinical question is whether the crack has reached the pulp which requires root canal treatment before a crown or whether it has extended below the gumline into the root, which changes the prognosis significantly.
4. Split tooth
A crack that has progressed to the point where the tooth has separated into distinct segments. A split tooth cannot be saved intact. Whether any portion of the tooth is salvageable depends entirely on the position of the split a crack confined to the crown portion may allow for partial retention, while a split that extends into the root almost always requires full extraction.
5. Vertical root fracture
A crack that begins in the root and travels upward toward the crown the reverse of a standard crack. These are the most clinically serious type because they produce minimal symptoms in early stages, allowing significant infection and bone loss to develop before the patient is aware of the problem. Vertical root fractures are diagnosed most often in root-treated teeth and almost always result in extraction.
Research published in the Journal of Endodontics notes that vertical root fractures account for approximately 11 percent of all extracted teeth a figure that reflects how frequently they are identified only at the point where saving the tooth is no longer viable.
How a Dentist Assesses a Cracked Tooth
The assessment of a cracked tooth is more involved than a standard examination because the damage is often not visible without specific diagnostic steps. Patients sometimes arrive expecting a single X-ray to give a definitive answer and leave frustrated when the dentist needs to do more. The additional steps are necessary, not excessive.
Bite test
The dentist asks the patient to bite down on a small plastic stick placed on individual cusps. Sharp pain on biting or more specifically, sharp pain on releasing the bite is the hallmark response of a cracked tooth. The location of the pain helps isolate which cusp and which part of the tooth is involved.
Transillumination
A high-intensity light is directed through the tooth. Cracks scatter the light differently than intact enamel, making fracture lines visible that would otherwise be undetectable. This technique is particularly useful for craze lines and early-stage cracks that have not yet produced symptoms.
Staining with dye
A temporary dye is applied to the tooth surface and then wiped away. The dye penetrates into cracks and remains visible after the surface is cleaned, mapping the extent and direction of the fracture.
Periodontal probing
A fine probe is used to measure the depth of the gum pocket around each root surface. A crack that has extended below the gumline creates a narrow, isolated deep pocket a reading that immediately signals the prognosis has changed.
Cone beam CT imaging
For complex cases particularly where a vertical root fracture is suspected three-dimensional imaging provides detail that a standard dental X-ray cannot. The additional cost is justified when the imaging directly determines whether a tooth is salvageable.
When the Tooth Can Be Saved
A cracked tooth is salvageable when the crack has not extended below the gumline, has not split the root into separate segments, and has not caused irreversible damage to the surrounding bone.
The specific treatment depends on how far the crack has progressed at the time of diagnosis:
Crown alone — for fractured cusps and early-stage cracks that have not reached the pulp. A crown covers the entire biting surface and prevents the crack from propagating further. This is the most straightforward intervention and carries a good long-term prognosis when placed promptly.
Root canal treatment followed by a crown — for cracks that have reached the pulp and caused pulpal inflammation or infection. Root canal treatment removes the damaged nerve tissue, eliminates the source of infection, and prepares the tooth to receive a crown. The crown is essential after root canal treatment because a root-treated tooth is more brittle and prone to further fracture without full coronal coverage.
Crown lengthening before a crown — for cracks that extend just below the gumline but not deeply into the root. A minor surgical procedure repositions the gum and bone to expose enough healthy tooth structure for a crown margin to be placed. This extends the zone of treatment without requiring extraction.
The earlier a cracked tooth is assessed, the more options remain available. A crack identified at the fractured cusp stage is a crown appointment. The same crack, left for twelve months, may be a root canal and crown or an extraction.
When Extraction Is the Right Decision
Dental extraction treatment becomes the appropriate clinical decision when the structural damage has passed the point where a restored tooth can function reliably or predictably.
The specific thresholds that indicate extraction rather than restoration:
A crack that extends below the crestal bone level — the point at which a crown margin cannot be placed with a reliable seal
A vertical root fracture — particularly in root-treated teeth, where the fracture has typically been progressing silently for months before diagnosis
A split tooth where both segments are mobile and no portion retains adequate bone support
Active infection with bone loss extending along the root surface, indicating the fracture has been present long enough to allow chronic bacterial colonisation
Extraction is also the more practical decision when the cost of saving the tooth — root canal, crown lengthening, and crown — significantly exceeds the cost of extraction and replacement, particularly where the long-term prognosis of the restored tooth is uncertain. A tooth with a guarded prognosis that fails two years after extensive treatment results in extraction anyway, at greater overall cost and discomfort.
This is not a comfortable conversation, but it is an honest one. A dentist who recommends extraction over a costly restoration with a poor prognosis is prioritising the patient's outcome over the revenue of the procedure. That is a sign of clinical integrity, not a lost opportunity.
What Happens After Extraction Replacing the Tooth
Extraction is not the end of the decision-making process. A gap left by an extracted tooth allows adjacent teeth to drift and opposing teeth to over-erupt over time, altering the bite and creating new problems. The Australian Institute of Health and Welfare notes that tooth loss in adults has measurable impacts on chewing function, nutritional intake, and quality of life — particularly when posterior teeth are involved.
Replacement options following extraction include dental implants, a fixed bridge supported by adjacent teeth, or a partial denture. Each carries different cost, maintenance, and longevity considerations. The dentist will discuss replacement timing and options at the extraction appointment — ideally before the extraction occurs, so the patient makes an informed decision about the full treatment pathway rather than discovering the options afterwards.
Frequently Asked Questions
Can a cracked tooth heal on its own?
No. Unlike bone, tooth enamel and dentine do not regenerate. A crack will not close or repair without clinical intervention. Without treatment, most cracks progress — either deepening toward the root or widening under the stress of normal biting forces.
How long can I leave a cracked tooth without treatment?
There is no safe waiting period that applies universally. A superficial crack that has been stable for years may remain so. A crack causing intermittent pain on biting is already producing symptoms that indicate structural involvement — every week without assessment is a week in which the crack may be propagating. The risk of waiting is that a restorable tooth becomes an extractable one.
Does a cracked tooth always hurt?
No — and this is what makes them clinically challenging. Vertical root fractures in particular cause minimal or no pain in early stages. The absence of pain does not indicate the absence of damage.
Will a crown fix a cracked tooth permanently?
A crown prevents further propagation of a crack that has not yet reached the root and distributes biting forces more evenly across the tooth. It does not repair the existing crack the fracture line remains. For cracks confined to the crown structure, a well-placed crown provides reliable long-term function. For cracks that have already reached the root, the prognosis depends on the depth of the fracture at the time of treatment.
If you have noticed sharp pain when biting that disappears quickly, a tooth that feels different under pressure, or a visible chip or crack along a tooth surface, an assessment sooner rather than later keeps more options open. Modern Dental Centre in Ballarat offers comprehensive examinations including digital imaging to assess cracked teeth accurately and clear, honest advice on whether saving the tooth or removing it is the right decision for your specific situation. Book an appointment online or call the team to arrange a time that suits you.



Comments